This Christmas, COVID-19 Was the Gift that Kept on Giving
Meanwhile, not only will New Year's Eve be wildly celebrated by the flippant tonight, but it's also a special somebody's birthday. That's right, COVID-19 is two years old today, and quite possibly about to enter its terrible-twos.
As stated by the epidemiologist and public health medicine specialist at the University of Melbourne, Professor Tony Blakely, shortly before festivities got underway,
We've got a superspreader event coming, it's called Christmas.
And that it was. Meeting and even exceeding expectations, this year's event-filled holiday season featured not only strangers but even friends and family passing on to each other the gift that keeps on giving, that gift of course being none other than the gift of COVID-19.
During this festive season in which millions of people have been paying it forward in record numbers (world-wide per day newly-reported cases on the 7-day average surpassed one million cases for the first time two days before COVID-19's second birthday), it can in turn also be expected that record COVID case numbers in country after country after country will mean an increasing number of health care systems will be overrun, more and more health care workers will be inundated with PTSD, more and more retail workers will be harassed by the shameless, along with all the other societal ills accentuated by dysfunctional polities.
In just the USA it's been estimated that more than 100 million people will be travelling as they year closes out, most of those people "done" with COVID and so effectively partaking in little to no safety measures besides the techno-solution of vaccinations, if even that. To make matters worse, and as if this couldn't have been seen coming a mile away, countless amounts of people have been getting stranded all over the world because the pandemic they tried to pretend is over actually isn't, an initial repercussion being thousands of flight cancellations all across the world due to the Omicron variant laying waste to flight staff.
Although the Omicron variant has yet to completely out-compete the Delta variant, it did however result in the Delta airline cancelling more than 300 flights over Christmas Eve and Christmas Day, with thousands more cancellations occurring in the proceeding days. For those whose flights weren't cancelled, and although the risk may have been low in the first place, Omicron bestowed the added gift of increasing the chance of catching COVID-19 on a flight by two to three times. (At least one woman, who tested positive while mid-flight between Chicago and Iceland, isolated herself in the toilet for the duration of the flight.)
"Good evening passengers, this is your captain speaking. After an unfortunate delay our flight will soon be embarking on its journey, so for safety purposes we ask you to please make sure both your seatbelts and your chin-warmers are securely fastened."
As summed up quite well by Tedros Adhanom Ghebreyesus, head of the World Health Organization (WHO),
All of us are sick of this pandemic. All of us want to spend time with friends and family. All of us want to get back to normal. The fastest way to do this is for all of us leaders and individuals to make the difficult decisions that must be made to protect ourselves and others.
In some cases, that will mean cancelling or delaying events. But an event cancelled is better than a life cancelled. It's better to cancel now and celebrate later than to celebrate now and grieve later. None of us want to be here again in 12 months time.
Putting aside the fact that these "normal" high energy-consuming times that "all of us want to get back to" are anything but normal in the grand scheme of things, at the rate things are going it's hard not to expect us being here again in 12 months' time, just as it's hard not to expect the lives of many loved ones being "cancelled" during these ostensibly joyous times.
That all being so, what better way then than to mark the occasion with a round of COVID investigations spiced up with COVID-themed adaptations of Christmas carol titles, investigations in which we can come together and revel in the myriad showings of "generosity" that we continue to witness in these "unprecedented times" we find ourselves in.
It's beginning to look a lot like another horrific variant of concern
Suffice to say, with the vast majority of the world's population actually believing that these are "unprecedented times" we're currently living in and that this isn't just the first significant stage in which industrial civilisation begins to implode in on itself, it should be of little surprise that most of us seem to have learned virtually nothing from the lessons that the Delta variant provided us and so still cling to the idea that the Omicron variant is not only "mild" but that it may actually be a good idea to have it spread. On the other hand, and as I mused a month prior to Christmas (before Omicron had been named),
While new revelations keep breaking by the day, it seems as if Omicron may not only be very (but certainly not extremely) bad but that we may want to count our lucky stars that it emerged after Delta, after the all the other previous variants had made their way around the globe, and after the subsequent vaccinations that we've managed to roll out so far. Because as it turns out, Omicron only appears to be milder than Delta.
For starters, not only is it looking like the Omicron variant may be "the fastest spreading disease known to man" (faster that even measles), but that over the next three months as many as 3 billion people (no, that wasn't a typo) may become infected with it.
That's obviously an extremely huge number (more than a third of the world's population), albeit one which may need to be toned down a bit in light of what may end up being an extremely fast initial rise in case count followed by an even more rapid crest (rather than the more usual long tail). Otherwise put, "[the] Omicron wave will be fast and intense across geographies, but is expected to burn through quickly."
We should be so lucky. Because while many have been trying to suggest that Omicron is "milder" than Delta – if not "mild", full stop – much of this has been based on poor information.
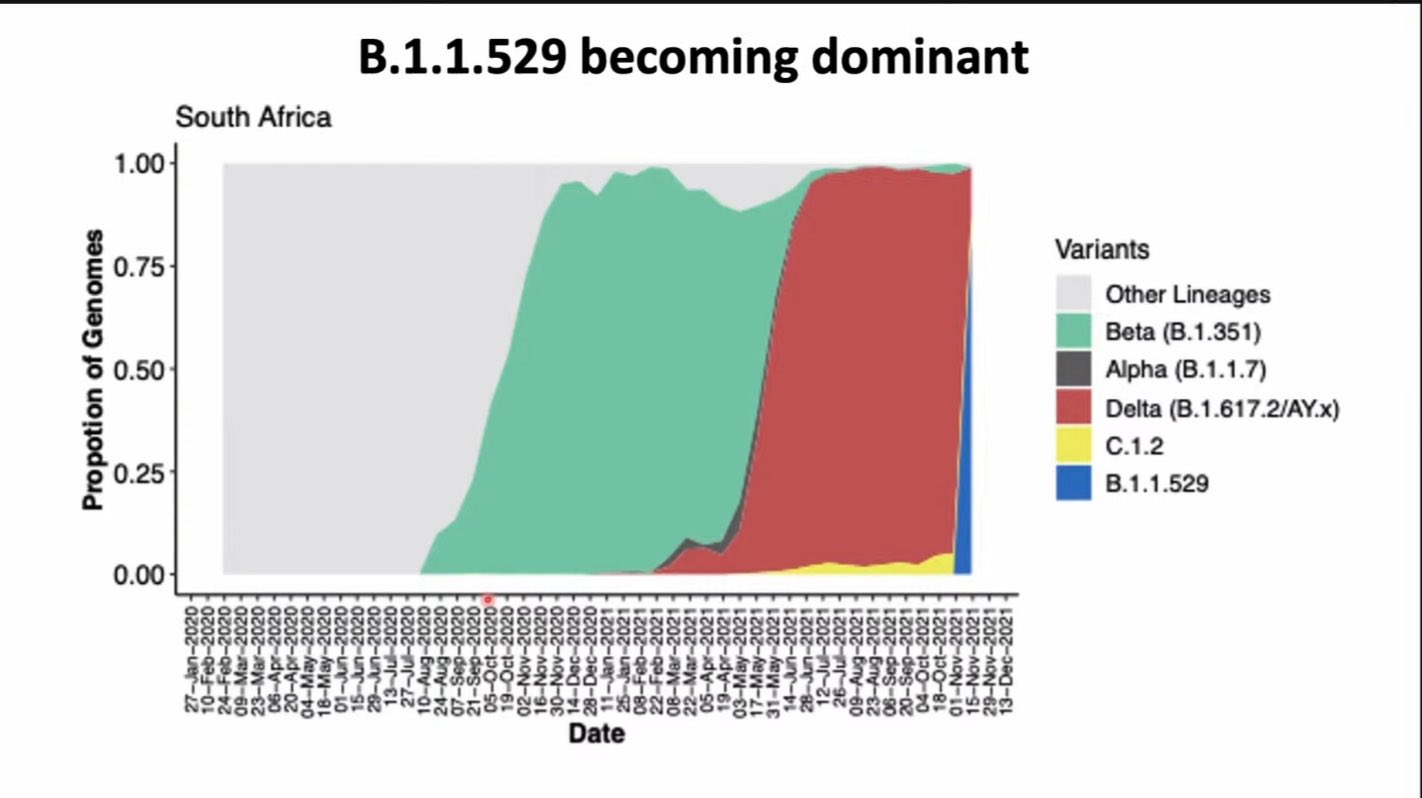
The first portion of poor information came courtesy of Dr Angelique Coetzee, Chair of the South African Medical Association. Coetzee gave interview after interview to international media outlets proclaiming that many of her colleagues were "seeing very, very mild symptoms and none of them so far have admitted patients to surgeries". Moreover, she not only continually repeated the words "very mild", but also continually argued against the need for any kind of restrictions. One problem here is that none of her assertions were based on any sort of scientific research but rather anecdotal evidence that she gleaned from a few sources.
Secondly, South Africa's median age is 27 (with less than 5% over the age of 60), much lower than the median ages in United States of 38 and in the United Kingdom of 40. Moreover, while that lower South African median age means less of a likelihood for individuals to be adversely effected by COVID-19, many in that age group would have also already been infected by the Alpha, Beta and Delta variants (many of those cases unreported) and so would have already built up a degree of natural immunity.
All of this means South Africa was in an ideal position to make the Omicron variant seem less severe than it actually is.
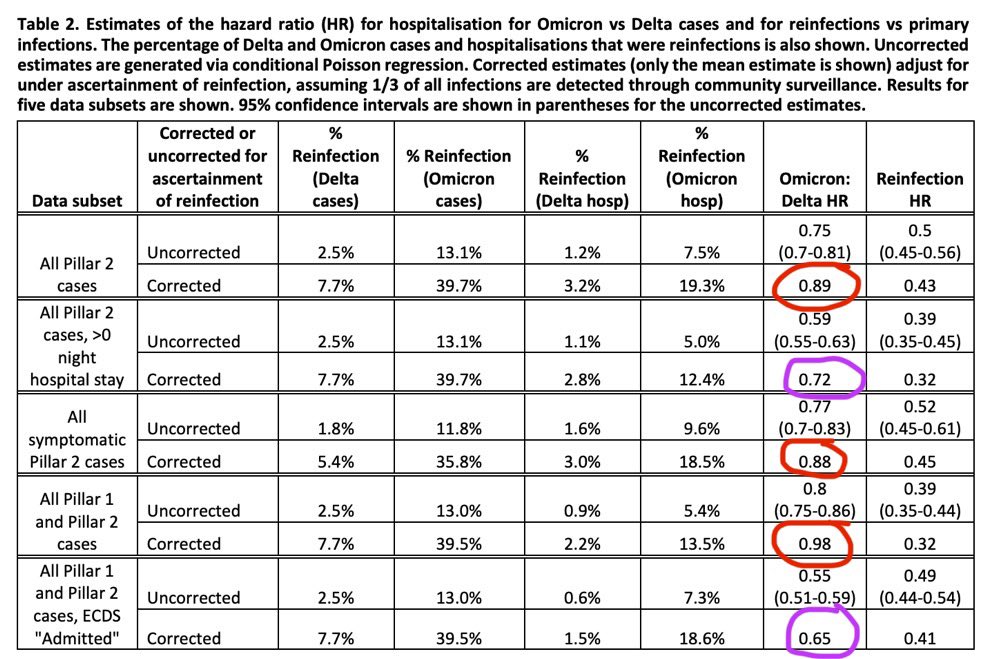
In place of anecdotal information the Imperial College of London undertook its own study though, results which are more than a bit concerning.
[T]he risk of reinfection with the Omicron variant is 5.4 times greater than that of the Delta variant. This implies that the protection against reinfection by Omicron afforded by past infection may be as low as 19%.
As it later states,
To put this into context, in the pre-Omicron era, the UK “SIREN” study of COVID infection in healthcare workers estimated that prior infection afforded 85% protection against a second COVID infection over 6 months.
To make matters worse,
The researchers found a significantly increased risk of developing a symptomatic Omicron case compared to Delta for those who were two or more weeks past their second vaccine dose, and two or more weeks past their booster dose (for AstraZeneca and Pfizer vaccines).
To reiterate, even if you've gotten a third shot of a vaccine you're still rather susceptible to getting infected (as the world over is seeing). To add some numbers to that disturbing detail,
Depending on the estimates used for vaccine effectiveness against symptomatic infection from the Delta variant, this translates into vaccine effectiveness estimates against symptomatic Omicron infection of between 0% and 20% after two doses, and between 55% and 80% after a booster dose.
As stated by OzSage, the independent Australian advisory group of experts in epidemiology, health and economics,
We know nothing yet of the incidence of long COVID associated with the Omicron variant. During the first wave in Sydney, one-third of people with mild-to-moderate COVID-19 were left with persistent symptoms, including shortness of breath and fatigue. Long COVID could impose an enormous economic and human cost on the Australian health system for years. New research from the US shows the virus persists in the brain, the heart, the kidneys and many other organs long after the initial illness, so preventing disease now may prevent long term chronic illnesses.
Although there's still a lot of unknowns involved, it's nonetheless been predicted by some that a massive wave of long COVID will begin to be seen in February of 2022.
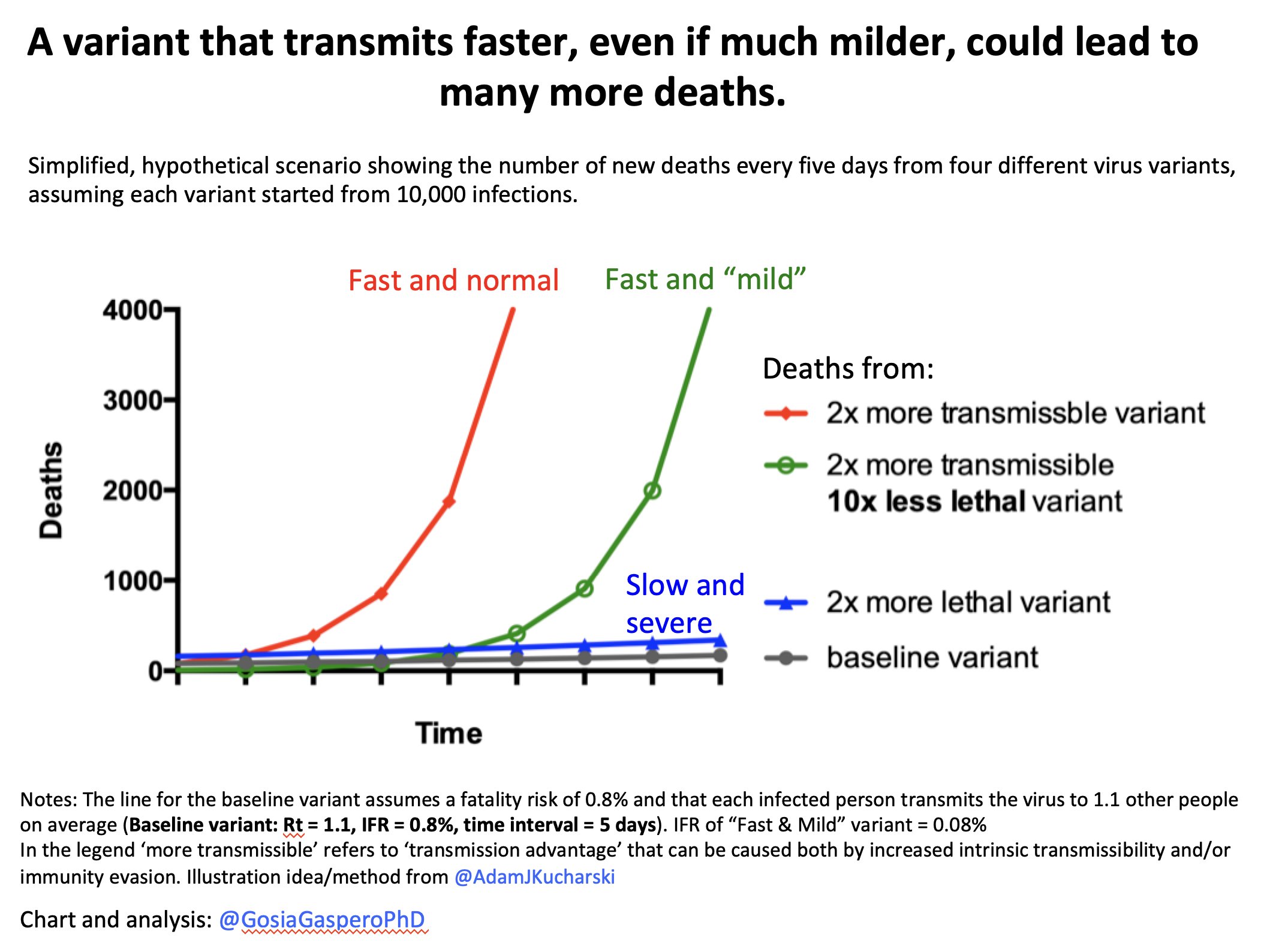
As if that weren't enough, the aforementioned extremely high transmissibility of Omicron means that even a small percentage of severe cases out of a very big number of infections would lead to a significantly high overall amount of severe cases, implying that waves of Omicron could very well result in similar amounts of hospitalisations and deaths as occurred during the heyday of the Delta surge(s). All of which, it needn't be added, would add further deterioration to what's left of our health systems.
All of that is of course contrary to the continual stream of feel-good reports emanating from most mainstream media outlets, pointing to various statistics that describe Omicron as being "milder" than Delta (which isn't necessarily saying very much considering the havoc Delta caused), if not just outright "mild", full stop. Never mind that this trope is being pushed by the usual coterie of scientists, politicians and journalists, but on closer inspection it would appear that the argument is based on little more than simplistic thinking, if not the turning of a blind eye to the data. Because what needs to be looked at is the intrinsic severity of Omicron versus its observable severity.
Described by Natalie E. Dean (assistant professor of biostatistics at Rollins School of Public Health), then expanded upon by Deepti Gurdasani (senior lecturer on epidemiology at Queen Mary University of London) as well as by Eric Feigl-Ding (epidemiologist & health economist who was also one of the first to ring the alarm about COVID-19), a new variant can simply appear to be less virulent even when there's no actual change in its underlying virulence (those three threads I linked to above are worth reading for a more thorough explanation than what I'll describe below).
In short, the original Wuhan strain was unleashed upon a worldwide population with no immunity whatsoever to SARS-CoV-2, while the Delta variant did at least have to contend with people that had at least a modicum of natural immunity thanks to previous infection(s) as well as those with varying degrees of immunity due to one or even two shots of a vaccine. Come late-2021, when large proportions of people in high-energy consuming nations have been vaccinated twice-over (and to a smaller degree infected once or more times or even had a third vaccination), the "playing field" that the nascent Omicron variant now has to contend with is very much changed.
Otherwise put, a large percentage of those not only potentially exposed to but infected with the Omicron variant already have a degree of immunity to COVID-19 thanks to prior infections(s) with COVID-19 as well as thanks to vaccinations. In turn, their varying degrees of immunity may not stop the emergence of mild symptoms, but will very likely prevent severe outcomes. Moreover, because Omicron is so capable of causing breakthrough infections of the vaccinated of which thanks to said vaccines are mostly "only" mild infections, these mild infections replace outcomes which would have otherwise been severe.
In effect, while it appears that Omicron itself is milder, it's actually the vaccines and immunity conferred from previous infections that is lessening the severity from Omicron. In other words, previous infections and vaccines are doing at least half decent jobs of keeping people "safe" (I put "safe" in quotations because there's no word yet on effectiveness of vaccines against Omicron-induced long COVID, be it with two or three doses of a vaccine).
With that understanding in mind, it turns out that Omicron may only be 2% to 12% intrinsically milder than Delta (which is, suffice to say, still very bad).
In effect, it might therefore be safe to say that humanity dodged a couple of bullets with the original Wuhan strain; (a) that the Wuhan strain was so mild in comparison to Omicron/Delta, and (b) that Delta spurred on so many people to hurry up and get vaccinated. Because if SARS-CoV-2 had of busted out of the gates and made its way around the pre-vaccine era globe back in early-2020 with the virulence of Omicron (just 2% - 12% less than Delta) and the measles-level transmissibility that Omicron has been said to have...
...WOAH.
The world would have been a significantly different looking place right now. Not apocalyptic, but certainly different.
(What this may also very well mean is that if Omicron enters pockets of families and/or communities who are not only unvaccinated but who have managed to avoid prior infection with COVID-19, watch out.)
So with two shots of a vaccine providing a modicum of protection against Omicron, if you haven't had your third shot yet it might be wise to get it as soon as it's made available to you (even though it's effectiveness at preventing symptomatic infections from Omicron begins to drop after 10 weeks, and even though its effectiveness against severe disease, which is more durable than effectiveness against mild infection, will nonetheless also decrease over time) while simultaneously maintaining other protective measures in order to try to ward off a rather easily attained "mild" infection (read: the possibility of long COVID). Suffice to say, not only did I snag my third shot Dec. 14th, but while I make sure to wear a KN95 or N95 mask while indoors, I do not patronise restaurants, bars, or cafés. As should go without saying, the virus doesn't take a break when you decide to.
First Pfizer shot, June 2nd, my birthday. Literally the first selfie I've ever taken in my life, which I royally screwed up. Didn't even know how to flip to the front camera. Second Pfizer shot, July 9th. I've learned how to switch to the front selfie camera, but don't quite have the timing thing down right. Third Pfizer shot, December 14th. I say "stuff this" and was able to get staff to allow a friend of mine to take the photo. Note: Yes, I am in fact wearing my Fanfare Ciocărlia t-shirt, rumour being that, with they literally being the fastest and most powerful band in the world, wearing their t-shirt while getting your COVID shot makes the vaccine work that much faster and stronger. Also, yes, I'm wearing a surgical mask in all three photos, which one is unfortunately made to wear instead of whatever you come in with. (Third photo by maker of F**k the Game)
Having said all of that, if there's any consolation that we might be able to extract from this quickly unfolding Omicron-disaster-in-the-making, that'd be that deaths emanating from this latest variant of concern may once again be in the millions rather than the tens of millions, the latter figure being closer to what might occur if SARS-CoV-2 does in fact end up mutating in one way or another into "the one we've all been waiting for".
Omicron is comin' to town
Back on August 27th the Danish health minister, Magnus Heunicke, stated that Covid-19 was no longer a "socially critical disease" and that all restrictions were to be removed by September 10th. Moreover, Heunicke added that "It is the good Danish epidemic management that makes this possible".
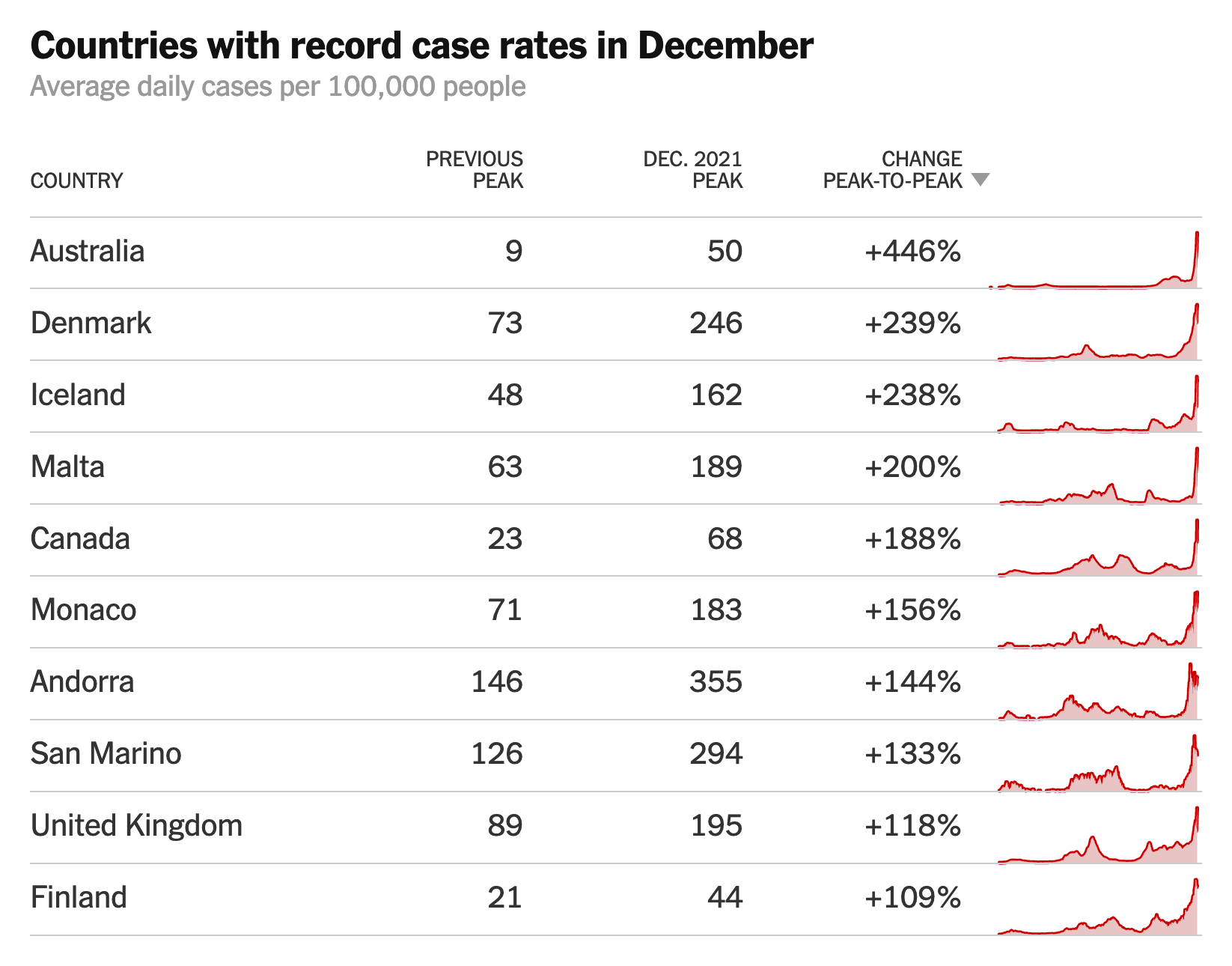
But with Denmark being one of the first countries to be hit hard with Omicron thanks to cases doubling every two days or so and case number records being set every day, Tyra Grove Krause, one of Denmark's chief epidemiologists, is warning that "The next month will be the hardest period of the pandemic".
That was no joke. By the end of December, Denmark had the highest recorded incidence of the virus in the world, with 1,612 cases per 100,000 people and deaths on the uptick.
To repeat: "It is the good Danish epidemic management that makes this possible".
Deck the halls with airborne COVID
Although 70 of 120 attendees of a party at a restaurant in Oslo, Norway came down with the new Omicron variant (as did another 50 people at the restaurant), 53 of 150 attendees at a lunch in Viborg, Denmark acquired Omicron (now at least 71), and 68 of 173 medics that attended a Christmas party in Malaga, Spain tested positive for Omicron, the event that takes the COVID-infused cake and which has been described as "one of the highest-transmission events this year in any single venue, probably anywhere in the world" is the case of the Argyle House nightclub in Newcastle, Australia in which more than 200 attendees out of 650 came down with the Omicron variant. Another 100 or so people then came down with Omicron after attending a Taylor Swift-themed dance party, clusters in the state of New South Wales (NSW) being driven by "super-spreading events at pubs and clubs". In fact, it's not just NSW but the entire world that has seen the young – those most likely to travel and socialise – jump-starting community spread of Omicron.
Similarly, and following a long procession of countries enacting inane COVID-19 restrictions, Ireland has become the latest country to (re)impose midnight curfews on pubs, restaurants and nightclubs, presumably because party-goers can only acquire COVID-19 if they eat and/or drink after the clock strikes 12.
Who deserves less respect? Somebody who doesn't wear a mask at all and so doesn't even bother to hide their narcissism/wannabee-narcissism, or somebody who tries to pass themselves off as if they actually give a shit about others by wearing their mask under their nose?
Regardless of where you stand on that, and supposing you cover both your nose and mouth with a mask, it's worth noting for those that aren't fully aware that cloth masks, particularly in light of the hyper-transmissible Omicron variant, are pretty much useless except for decorative purposes. They may do a half-decent job of protecting others from your exhalations, but they do little to protect you from breathing in contaminated air. Likewise for disposable surgical masks that leave gaps all along the sides.
In short, if you want to be properly protected then get yourself a respirator – an FFP2 (in the EU/UK), an N95 (USA), a KN95 (China), or a KF95 (South Korea). As stated in a Twitter thread by Ali Nouri (a molecular biologist but also assistant secretary at the U.S. Department of Energy, so I assume we'd disagree on many energy issues) that has more detailed information in a few links,
Back in early-November the Singaporean government, which currently covers the medical costs of all its citizens, announced that it was going to start charging patients that were "unvaccinated by choice" for their COVID-19 treatments. Singapore, like pretty much all other highly-vaccinated countries, was finding that the vast majority of those ending up in hospitals with COVID-19 were, unsurprisingly, the unvaccinated, placing an undue burden on health systems and on health care workers that are increasingly demoralised and burned out.
Case in point, of the 115 ICU patients in Melbourne and the rest of the state on Christmas Day 94% were unvaccinated, while most of the 6% that made up the vaccinated had underlying illnesses or compromised immune systems. And like Singapore, not only are staffing crises of all sorts are hitting Melburnian hospitals, but overcrowded hospitals and staff that are spread too thin have meant more than just delays for non-essential surgeries. As stated by Omar Khorshid, president of the Australian Medical Association, prior to Omicron hitting and causing rapidly increasing record case numbers in Sydney and the rest of NSW,
You probably don’t want to have a heart attack or be diagnosed with cancer in October in NSW, and really we need to do everything we can to avoid our hospitals suffering from opening up too early.
To little surprise, and in what seems to be his Christmas present to Sydneysiders and everybody else in NSW, on Dec. 23rd the health minister of New South Wales' libertarian Liberal government, Brad "the bio" Hazzard, admitted that the state government was considering charging unvaccinated patients for their medical bills. This would be, it should go without saying, contrary to Australia’s system of universal healthcare.
Although Khorshid obviously had issues with overrun hospitals, he nonetheless made no qualms with criticising what would be a radical departure from norms in Australia.
The big issue from a medical point of view is that it's really not ethical or the right thing to do to limit access to healthcare based on people's previous health choices.
If you follow that same logic, are you going to ask smokers to pay for their healthcare?
I think it would be a real shame if through this pandemic we lose our compassion, we lose our humanity, and our care for fellow Australians, even if they've made choices we think are unwise or incorrect or even completely antisocial.
No doubt many people have become exhausted with the merry-go-round of variants of concern and the incessant COVID crises they bring along (Omicron's arrival occurring in the midst of holiday season, no less), and no doubt the idea of enacting revenge upon anti-vaxxers for their narcissism and their disregard for the well-being of others is a tempting option that would resonate with some, if not many, particularly when one in five of those who died of COVID during NSW's Delta surge caught it while they were in a hospital for an unrelated reason.
But even though immense pressure is being placed on health systems, has pushed hospital systems to the brink, has furloughed countless staff due to exposure, and has once again shut down elective surgeries, it's important to note that the act of charging anti-vaxxers for their COVID-19 medical bills is actually a Trojan horse for bringing in the privatisation of healthcare and the destruction of Australia's public healthcare system. The threat of charging the unvaccinated for their COVID-19 bills isn't about using "the stick" to try and convince the hesitant and resistant to accept vaccination, it's about the ideology of transforming Australia's healthcare system into something akin to the United States' dysfunctional "everybody for themselves" system.
That all being said, it is of course absurd that people who don't trust COVID-19 vaccinations because they "don't know what's in them" simultaneously feel perfectly fine calling an ambulance and checking themselves into a hospital when they catch COVID, all the while allowing themselves to be injected with a plethora of medicines of which they just as well have no idea what they're made up of.
So although it would be wrong – while also falling for a trap – to charge the unvaccinated for their COVID-19 medical bills, and short of triaging anti-vaxxers to the broom closet when a vaccinated person needs emergency medical attention from an overloaded hospital, would it be so wrong for said anti-vaxxers to have at least a modicum of respect for those making the minimum of effort to protect themselves with a vaccine by making it a point to not admit themselves to the hospital when they catch COVID-19?
Yes, Rudolph and his symptomatic nose may very well "go down in history", although if we're lucky enough it'll be for super-spreading COVID-19 to no more than all of his mates across an entire continent. Let's back up a bit to better understand this.
For starters, COVID-19 is of course zoonotic – it can spread between animals (most famously bats and pangolins) and people. It doesn't stop there though, as it's been confirmed that in early 2020 COVID-19 was in fact passed on to a cat from its owner. As stated by Margaret Hosie, professor of comparative virology at Glasgow University, upon discovery of the infected Siamese cat,
If you have any respiratory signs, then be sure to catch your cough or sneeze into a disposable tissue, and wash your hands before you handle your cat. Don't kiss your cat. Don't have the cat sleeping in a bed with you, and don't share food with the cat.
Which can probably be summed up with the single sentence "Please don't be a disgusting idiot", seeing how cats not only carry various diseases themselves, but because like dogs they also lick their assholes.
To be more specific, it's not the health of the infected cats that we should be worried about so much as the blowback. As explained by Dr Els Broens of Utrecht University in the Netherlands,
The main concern, however, is not the animals' health – they had no or mild symptoms of Covid-19 – but the potential risk that pets could act as a reservoir of the virus and reintroduce it into the human population.
It's so far been our fortune that that has yet to verifiably occur with any animal, except, that is, for mink.
Most notably in Denmark (but also in Italy, the Netherlands, Spain, Sweden, Poland, France, Finland, Canada, Greece, Lithuania and the US) was the observed transmission of COVID-19 from humans to farmed mink. While thousands of mink died in Utah alone (mink experience the same respiratory distress as humans do from COVID-19), a new coronavirus strain emerged in Danish mink which led to fears of decreased efficacy rates of vaccines in humans. Although more than 200 Danes were infected with mink-related variants, fears of a much more dangerous variant have not eventuated. Nonetheless, Denmark, which used to be the world's top exporter of mink furs, culled 17 million mink after outbreaks at more than 200 farms. (Later on several million of those mink had to be dug up and incinerated when gas from their decomposing bodies caused them to rise from their shallow graves and in turn threaten nearby waters.)
That's a lot of mink... down the sink
Since "minkgate", not only have many more cats (and eventually dogs) tested positive for COVID-19, but 13 gorillas in an Atlanta zoo caught COVID-19 (likely from a zookeeper), two endangered snow leopards at the San Diego Zoo tested positive (several snow leopards later died at various other zoos across the US), two hyenas, 11 lions and two tigers at the Denver zoo tested positive, three tigers tested positive at the San Diego zoo (even though they'd already been vaccinated, as had hundreds of other animals at the zoo), two hippos tested positive in Belgium, and on and on it's gone. In fact, while many animals at zoos have been vaccinated, Finland is now vaccinating hundreds of thousands of mink.
We've always recognised that coronaviruses have this tremendous capacity to jump species. So it was always predicted that there would be a variety of domestic animals, livestock and potentially wildlife that could be infected.
You could be concentrating on eradicating the virus in humans, but meanwhile the virus could be mutating away quietly in an animal species, and getting hotter and hotter.
So while the roughly 18% of pets belonging to COVID-19 patients that have tested positive are animals that don't transmit to humans (so far?), what does have many scientists rather concerned is the prevalence of COVID-19 in Rudolph's colleagues.
In May of this year a report in the Journal of Virology conveyed the fact that white-tailed deer, native to North, Central and South America, "are highly susceptible to infection" of COVID-19. Just two months later researchers at the US National Wildlife Center in Fort Collins relayed the finding that roughly a third of white-tailed deer in the US north-east had antibodies to SARS-CoV-2 (which doesn't necessarily mean they were infected, as antibodies can indicate having fought off infection), while a more recent study showed that 40% of white-tailed deer had detectable antibodies. But just last month a more concerning study showed that roughly 80% of white-tailed deer tested in Iowa (via the lymph nodes of road kill and those felled by hunters) between November 2020 and January 2021 "had detectable SARS-CoV-2 RNA". In other words, these, on the contrary, were in fact active infections.
While rampant deer-to-deer transmission has quite obviously occurred there's no evidence that any deer have become sick with their infections. With the amount of samples available scientists have nonetheless been able to genetically sequence a number of variants present in the deer, variants which matched various variants circulating in humans at the time – suggesting that not just one but several human-to-deer transmission events have occurred. Although it's been theorised that deer could have been infected from humans through sewer discharge, through the licking of tobacco spit out by an infected hunter, during various wildlife management operations, field research, recreation and tourist activities, etc., there is however no conclusive evidence of how transmission has ever occurred.
No deer, please don't kiss the dear
Regardless of how deer have become infected, what's instead instilled many scientists with dread is the fact that a large reservoir of SARS-CoV-2 now exists in not only a wild animal, but in North America's most populous game species. The fear, of course, is that like the occurrence in mink whereby COVID-19 was able to mutate and then pass back into humans, the virus will become endemic in deer, evolve to become more virulent, then re-infect humans while also being able to evade current vaccines. At the present time there is however no evidence of deer-to-human transmission having ever occurred. (Nonetheless, a popular theory is that the new Omicron variant came courtesy of a reverse zoonotic event – that is, it evolved in an animal and made its way back to humans at some point.)
What this all means is that even if we were to somehow eradicate COVID-19 in the entire human population the virus would still have a safe haven in which it could continue to circulate, create new strains, and possibly spill back into humans. Suffice to say, eradicating SARS-CoV-2 from wild deer, which number 30 million in the US alone, wouldn't exactly be an easy task. Otherwise, and as stated in a Naturepaper published on Dec. 23rd,
[T]hese findings demonstrate that SARS-CoV-2 viruses have the capacity to transmit in US wildlife, potentially opening new pathways for evolution. There is an urgent need to establish comprehensive “One Health” programs to monitor deer, the environment, and other wildlife hosts globally.
Fortunately, besides hunters who have been warned by the CDC to take various precautions when dressing and processing deer (and to cook all meat to at least 75°C), the fact remains that humans don't spend much time breathing in the same air that deer do.
But following a quote by Rebecca Fisher (an assistant professor of epidemiology at Texas A&M University) in which she reiterates the aforementioned concern about animal-to-human transmission, The Guardian then stated the following:
[Fisher's] greater fear is the virus adapting to wild animals that live in close proximity to humans, such as rodents. Fortunately, rats and mice don't appear particularly susceptible to Sars-CoV-2 infection at the current time.
That was stated and published on December 11th, and oh how things can develop with this COVID-19 shit show. Because it was just three days later, on December 14th, that a preprint revealed that although previous variants of concern had little ability to bind to rodent ACE2 receptors (the entry point for SARS-C0V-2 in humans and other animals), the Omicron variant has now changed that – "Omicron appears to have gained the ability to bind to rodent ACE2".
Although rats may not have been the underlying factor of the Black Death's spread in mid-14th century Europe (which killed off a third of the human population), now might nonetheless be as good of a time as any to stop cavorting with rats and slipping them the tongue.
Does purple hair on rats simply mean they've been died with Kool-Aid, or that they're positive for a wickedly mutant strain of COVID-19?
12 days of quarantine
Yes, there was a time here in Australia when people in many states would fret when case numbers rose all the way up to three or so. No, not three thousand, or even three hundred, but three, full stop. Those days are now well and truly gone for all Australians (bar those in Western Australia, which may very well retain its isolation beyond its stipulated February 5th re-opening date), the country quickly becoming another cesspool of COVIDity that Rupert Murdoch and his newspapers have so very much craved and worked towards for the past two years.
This quickly emerging shit show started earlier this year when the libertarian and astonishingly arrogant then-premier of NSW, Gladys Berejiklian, refused to follow along with New Zealand's and the rest of Australia's successful examples of locking down hard and fast in order to crush an outbreak of the Delta variant, Berejiklian deliberately choosing to ignore the medical advice of the chief health officer of imposing Victorian-style lockdown measures. (The index case of a limousine driver had been quickly identified, although rather than crush the outbreak it was effectively allowed to proliferate by Berejiklian, Berejiklian's response instead being to shift the blame to the limousine driver, a driver that had followed the very rules that Berejiklian's government had enacted but whom authorities nonetheless tried to have charges placed against. [He was later exonerated.])
To make matters worse, said outbreak of the Delta variant, which spread across NSW and Victoria (which other states like Queensland and Western Australia were able to successfully eradicate via hard and fast lockdowns on the multiple occasions that it leaked across their borders) was effectively spurred on by prime minister Scott Morrison when he commended his fellow Liberal party member Berejiklian for resisting to go into full lockdown and for being the "gold standard" of COVID-19 suppression.
When cases exploded in NSW Morrison excused Berejiklian by stating no one could see the severity of the Delta wave coming, even though Morrison himself had just earlier imposed restrictions on flights from India due to an outbreak of the very same variant. (As the world is now readily aware courtesy of French president Emmanuel Macron, Morrison is a serial liar who spits out as much detritus as the country's prized bullock.)
Berejiklian too made the same excuse of claiming ignorance of Delta's strength, even though she'd earlier stated that she felt "devastated about the COVID situation in India" and for people to "Please know NSW stands by you during this difficult time". No doubt it's nice that Berejiklian felt such concern for India that she was willing to stand by it in it's difficult time, but it's rather unfortunate that Berejiklian had no interest in standing by the people of NSW – and by extension the people of Australia – in their trying time of Delta-imposed difficulty.
The outbreak relegated NSW and Victoria into months of agonising lockdown (with rabid attendant protests spurred on by the Murdoch press), the Morrison government's incompetent procurement and thus belated roll-out of vaccines ("strollout" was chosen as Macquarie dictionary’s 2021 word of the year) necessitating those lockdowns lest NSW and Victorian hospitals collapse under the weight of overrun systems.
Following NSW's reprehensibly late lockdown and Victorians' inability to properly adhere to yet another extended lockdown (due to understandable lockdown fatigue after the previous year's 112-day lockdown) COVID-zero was not practically achievable in either state, setting the stage for not only the libertarian wet dream of "living with COVID" but the incendiary allowance for Omicron (and inevitably any and all subsequent variants – beware!) to enter the country.
If there ever was an example of how to not play to your advantage, and how to not only consciously and systematically throw it all away but how to go from being one of the world's shining lights to an utter shit hole of COVIDity, Australia, an island nation – a f***ing island nation! – is its personification. (On the other hand New Zealand appears to be inching its way back down to zero cases, although whether it actually plans to try and keep it that way is another story.)
And now? Well, suffice to say the Omicron variant has been welcomed into Australia with open arms, much of the country quickly falling into various forms of disarray (and then more disarray).
For starters, and with the Morrison government having opened Australia's international border to not only Australians currently overseas but also students and those with work visas, the country's largest states, NSW and Victoria, have announced in tandem that vaccinated international arrivals will no longer have to quarantine for even the watered-down 72 hours (goodbye 14 days, let alone 12 days of quarantine), requiring little more than a negative pre-departure test within three days of boarding a flight as well as a PCR test within 24 hours of arrival, isolation only required until a negative result is received (while for performative's sake another negative result is also required later in the week). That all being said, on the day before New Year's Eve Dominic Perrottet, NSW's new premier, announced that the state was scrapping PCR testing for vaccinated international arrivals altogether.
Meanwhile, while NSW has largely scrapped genomic sequencing and so to a large degree is riding blind when it comes to understanding the prevalence of Omicron (or a new off-shoot variant), the requirement for masks has also been mostly scrapped, simultaneously exploding case numbers being testament to the state now being as close as can be to "letting it rip" with high vaccination numbers. (Victoria extended a few masking and vaccination requirements on Dec. 15th – the day they were set to expire – then increased masking requirements to all indoor settings on Christmas Eve day.)
To add insult to injury, prime minister Morrison is now giving Rupert Murdoch what his newspapers have been clamouring on for for the past two years.
We're not letting Omicron take us back. We've decided as a country to live with this virus and Australians have worked so hard for that. Australia can now open up. This Christmas we’re about to have is a gift Australians have given to themselves by the way they’ve worked together with the settings that we've put in place.
Scott Morrison's Christmas gift to Australia (image via The New York Times)
It shouldn't need to be said that "live with the virus" actually means die with the virus, if not just live with the virus that makes your body attack your brain cells which then don't grow back.
We're going to live with this virus not let it drag us back where we've been ... We've got to keep moving forward, we can't slip back.
Of course "back" in the day Australia had achieved COVID-zero (like Western Australia continues to maintain), while going "forward" appears to mean no less than turning Australia into a COVID-riddled shit hole like the USA, or better yet like the UK which also threw away the advantage that comes with being an island nation.
If we do that, then we can keep our nerve, keep calm and carry on.
In case you've forgotten, crown, one of which can be seen at the top of this image, is the English translation of the Latin word corona
Sure, Morrison can claim (to his faux national cabinet) to be against harsh measures –
One of the main things we agreed on today is, we do not want to go back to lockdowns.
– but his libertarian ethos is all but certain to send Australians straight back into (Omicron-flavoured) lockdown as hospital systems across the country begin to buckle and collapse under the weight of Rupert Murdoch's and Scott Morrison's Christmas gift to they country.
Veering off into the absurd, Morrison has since tried to justify inflicting COVID-19 upon Australia by likening wearing masks to applying sunscreen, suggesting that such decisions were ultimately up to personal responsibility. Never minding that that's one of the dumbest analogies around since sunburn isn't airborne and therefore contagious, but it's an even worse analogy since personal responsibility doesn't work at the society level, which is how pandemics are best dealt with.
Veering off into the absurd, Morrison then likened wearing masks to applying sunscreen, suggesting that decisions as such were ultimately up to personal responsibility (something that doesn't work at the society level, which is how pandemics are best dealt with).
In the same way as we go into the summer season, people will be slapping on the hat and slapping on the sunscreen. There's no rule or requirement to do that, but it is strongly recommended health advice. [Wearing a mask] is in the same category.
But it's not at all, Morrison's analogy being one of the most asinine one could come up with. Wearing sunscreen does in fact protect yourself but it does not protect others due to the fact that COVID-19 is an airborne contagious virus, whereas wearing a mask does in fact protect you and others.
But even though the Australian Health Protection Principal Committee (AHPPC) suggested that "Implementation of mask-wearing measures should occur prior to Omicron case escalation to have maximum benefit", and even though Australia's chief medical officer professor Paul Kelly stated the same – "The health advice is wear a mask" – all Morrison could muster was the limp and ineffectual argument that "What matters is that people wear them, not whether people get fined or not".
But of course mandating masks isn't about threats of fines but is about displaying that the government puts credence on those with the best information and acts on that information. In effect, it's fair to say that Morrison is fine lecturing Australians about responsibility, but has no interest in partaking in the responsibilities of a prime minister who would thus be following the advice of the country's top medical advisors.
Victoria's chief health officer, Brett Sutton, put it best when asked about whether or not masks should be mandated.
The difference between highly recommending something and mandating something is the level of compliance that we see. I have just pointed out to you the masks that we saw come off as soon as we went from mandate to strongly recommended. We usually get about 50% levels of cooperation or compliance with a strong recommendation. It goes to 95-99% with a mandate. Why would you introduce a half measure when you need the full measure to be in place?
Why indeed.
But until the last minute NSW premier Dominic Perrottet was having none of it, all but completely parroting the libertarian ethos of Morrison, arguably outlining how his and Morrison's libertarian Liberal governments are running a confidence scheme.
It is a time of personal responsibility for our state. We are treating the people of our state like adults. I completely accept that people are concerned. But it is our job as a government to provide confidence. There will always be new variants of this virus. The pandemic is not going away. We need to learn to live alongside it.
Meanwhile, and in parallel to the utter shit show in England, people in NSW are now being asked to do their own contact tracing, most of those under 50-years-old are advised to manage their COVID at home, if help is needed people are advised to call their GP (even though most practices are operating on skeleton staff at this time of year), and people are being encouraged not to line up for PCR tests, all of which resulted in Omar Khorshid stating that "they’re almost abandoning their population to COVID."
Not "almost", it's exactly what they're doing. It shouldn't need to be said that the Doherty Institute Modelling Report for National Cabinet (the basis of the plan for states to open up once the critical percentage of 80% of eligible people had received two doses of a vaccine) was based on the Delta variant being the active strain in the country. But since vaccines which performed rather admirably against Delta perform rather poorly against Omicron, the new parameters completely invalidate the Doherty Report's modelling and in effect imply that the "80% vaccinated" line of defence has not only been compromised but has been utterly invalidated. With federal and state governments nonetheless championing for Australia to "open up" and "live with the virus", along with repeatedly claiming how mild Omicron is and that infections are inevitable for everyone, governments are no longer partaking in any kind of public health strategy, have abdicated their responsibility to their citizenry, and are actively excusing their inaction by shifting to a policy of mass infection.
It wasn't even two weeks after advising those 50 years-of-age and under to manage their COVID at home, that upon NSW's hospital system continuing to deteriorate and become overloaded the age bracket of those told to self-manage their COVID infections at home was raised from 50 to 65 years of age.
All of which is "a recipe for disaster" Khorshid also says, and that "by the time hospital admissions and ICU cases grow beyond whatever benchmark [Perrottet] is working to – it will be too late."
Because if there's anything we've learned these past couple of years (particularly from NSW's allowance for the Delta variant to proliferate) it's that it's necessary to get ahead of the virus in order to implement effective measures that prevent hospitalisations, reduce transmission, and in exceptional circumstances can even return states – and even countries – back to COVID-zero. In short, the precautionary principle rather than waiting to see if things actually get bad, at which point it's largely too late to rein things back in. Shining examples of the kind of action to undertake include the state of Tasmania which mandated masks indoors after recording only seven cases, and especially Western Australia in which premier Mark McGowan mandated masks indoors after a single case was detected after it managed to squeeze into the state at the last minute from Queensland.
That all being said, a few days before this post went live the Perrottet libertarian Liberal government in NSW did in fact re-mandate masks after horrendously sky-rocketing case numbers seemed to enlighten Perrottet as to what exponential growth is, mandates which unfortunately weren't enacted before the virus had a chance to seed itself deep within the state's populace, destined to also wreak havoc across most if not all of the country.
All in all, if you want to sum up in one sentence the libertarian notion of "personal responsibility" promoted by prime minister of Australia Scott Morrison and premier of New South Wales Dominic Perrottet, it's this:
Please make sure you've taken personal responsibility for yourself by pre-booking an Uber to drive your dead, COVID-riddled body to the morgue.
Otherwise, RIP Australia. Because when it comes time to dealing with the very possible upcoming variant of concern that might very well make the combination of Wuhan + Alpha + Beta + Gamma + Delta + Omicron look like a walk in the park, it now appears all but inevitable that it'll not only be welcomed into Australia with open arms, but that, unless McGowan decides to maintain Western Australia's isolation from the rest of the country, it'll be allowed to proliferate from coast to coast as it sees fit.
Because as University of Sydney infectious diseases paediatrician Robert Booy summed it up,
We are now ideologically driven and the public health advice has become secondary.
On the bright side, at least Rupert Murdoch is now happy.
As far as it's seen by professor Blakely (whose quote started off this post), "In broad-brush terms, there are two pathways out of this pandemic".
First, we continue to suppress the virus to low levels, and wait for better vaccines. Maybe by mid-2022 we will have new vaccines that are much better than current one[s] against Omicron (and future variants), and not only protect against serious illness but also greatly reduce the chance of any infection. And it is game-back-on to try to achieve that illusive herd immunity through vaccination alone.
... While I would be delighted if such vaccines arrive, I suspect it unlikely in the next six months.
Well, believe it or not, there may very well be such a vaccine that will emerge for public usage sometime in the next year or so. According to a news release by Defense One, scientists at Walter Reed Army Institute of Research will soon be announcing the development of their Spike Ferritin Nanoparticle (SpFN) COVID-19 vaccine that purportedly protects against all COVID-19 variants, including Omicron (and even SARS as well).
Working off of a DNA sequence of the COVID-19 virus that it received in early-2020, Walter Reed researchers made the decision to work on a vaccine that would work against all potential variants, utilising what is described as a soccer ball-shaped protein. Although phase 1 of human trials are wrapping up, the vaccine will still need to go through phase 2 and 3 trials.
But that's by far not the only option being worked on. According to the WHO there were nearly 300 different vaccines in development in mid-2021 of which ranged from patches to nasal sprays to pills to needle-based injections to needle-free spring-powered injectors, etc. (105 of those were in the human-trial phase and 184 were in the pre-clinical phase). Two of these being worked on in Australia are another set of variant-proof vaccines, vaccines whose methodology is to target stable portions of SARS-CoV-2 rather than the spike proteins of unique variants.
The current crop of mRNA vaccines, initially designed for the original Wuhan strain, target the spike proteins which to varying degrees change when the virus mutates from one variant to the next, simultaneously incurring another variability of reduced effectiveness upon vaccines. (If I may put on my tin-foil hat for a moment, sure, Pfizer and Moderna's methodology of targeting spike proteins may have been the relatively easiest approach to initially undertake, but simultaneously also the most monetarily lucrative approach to undertake if variants were able to keep changing their spike proteins and thus required routine boosters and/or updated vaccines catered to said new variants – possibly three injections per year!)
On the other hand, if a vaccine were able to target a portion of the virus which couldn't change structurally (lest the virus no longer be effective), then it would work against all current and future variants. More than two dozen pancoronavirus vaccine projects are being worked on around the world, including via the cutting-edge but now somewhat blasé mRNA methodology, novel nanocages arrayed with viral particles, as well as the more traditional cocktails of inactivated viruses, all of which are added to by such things as a vaccine based on the smallpox vaccine, the only deadly disease that's ever been eradicated.
To heap on even more news to amplify those happiness chemicals in your brain, according to Eric Feigl-Ding "the SpFN trial was conducted by Walter Reed in collaboration with the Henry Jackson Foundation for Military Medicine – which is a 501c3 nonprofit", suggesting that the vaccine's intellectual property rights might be held in a non-profit manner.
Whether or not such a possibility pans out, the fact that it'd be welcomed as good news is due to the fact that there are those who for more than a year now have been calling for a TRIPS waiver (the waiving of intellectual property rights for COVID-19 vaccines, which has been held up the likes of Australia, the UK, the EU, and a few others), inclusive of those such as former UK prime minister Gordon Brown, economist Joseph Steiglitz, and most notably of all, The People's Vaccine organisation.
As The People's Vaccine quite justifiably likes to say in their call for a vaccine "freely" available to all, "We cannot donate our way out of this pandemic", a sentiment proven by the dismal leftovers, castaways, and even soon-to-expire doses (that had to be dumped by Nigeria) that energetically wealthy nations have been handing over to energetically poorer nations (of which have received 0.6% of all vaccines), as well as by what seems to be a continual stream of new variants of concern that keep spinning out of highly-unvaccinated countries.
It's for these reasons and more that The People's Vaccine likes to point to a Human Rights Watch study showing that more than 100 firms across the world have the potential to make mRNA vaccines. Likewise, The New York Timespublished a list of 10 potential mRNA manufacturers, although as Omicron is now showing us The New York Times' description of mRNA vaccines as "the gold-standard" seems to be about as brilliant as Australian prime minister Scott Morrison's description of Gladys Berejiklian's Liberal-led libertarian NSW government as "the gold standard" of dealing with COVID-19.
In fact, it's questionable how useful these first-generation mRNA vaccines by Pfizer and Moderna now are, considering that not only are we playing whack-a-mole with these destructive new variants that keep popping up, but that the variants are mutating faster than vaccines can be adapted, produced, distributed, and administered. With both Moderna's CEO and Pfizer's CEO saying that it'll take about 100 days for them to develop and ship an Omicron-adapted vaccine, many voices, including that of a Singapore doctor Leong Hoe Nam, find it hard to see the point.
Nice idea, but honestly, it is not practical. We won't be able to rush out the vaccines in time and by the time the vaccines come, practically everyone will be infected [with] omicron given this high infectious and transmissibility.
Already we're seeing the hyper-transmissible Omicron variant traverse the globe and infiltrate regions with unparamounted speed and ease, and with an Omicron-adapted mRNA vaccine not ready to be shipped until early-March at the earliest, it'd then take another several months on top of that for it to be administered to a significant amount of people (in the wealthier parts of the globe, I might add). What would the point then be if, in the middle of that rollout, yet another variant popped up which rendered the Omicron-adapted vaccine just as half-arsed as the original Wuhan-catered vaccine was to Omicron?
Regardless of the futility of the cat and mouse game being played with these first-gen mRNA vaccines (which is not intended to be a back-handed excuse for vaccine inequity and the poor getting left high and dry), another statement that The People's Vaccine likes to make is that "No one is safe until everyone is safe". The suggestion behind this statement is that until the entire world's population is vaccinated there's still going to be ample opportunity for new variants of concern to come along, theoretically with the ability to evade vaccine-induced immunity (as well as natural immunity) and thus sending the world back to square one.
Part of the problem with this though is that even if enough vaccine was able to be produced for the entire world's population, and made available to all freely (so to speak), and could be administered across the world within a month or so in order to avert new variants of concern popping up from the not-quite-yet vaccinated while the rollout is underway (which could render the so-called People's Vaccine useless), there's also the fact that a considerable size of the world's population absolutely doesn't want to get vaccinated (even if God-man Trump tells them to).
Sure, some countries are now mandating vaccines for all of those eligible, Ecuador being the latest, but it remains to be seen how that would be practically possible. Does the Ecuadorian government plan on physically restraining people while the authorities force injections into them? Try forcibly injecting somebody in the United States (where a dismal 62% of those eligible are "fully vaccinated" with two shots) and there's a good chance they're gonna turn around and inject you with some lead (all the more easier with gun purchases and first-time gun ownership rapidly accelerating in the US during the pandemic).
Returning to professor Blakely, there's also the second pathway he wrote of in terms of getting out of this pandemic, written on December 20th and referencing a study published on August 25th.
The second general pathway out of this pandemic is a messier one – using both vaccines and natural infection to get to something like herd immunity. A study from Israel found that an infection with a pre-Delta variant was 13 times better than two doses of Pfizer at preventing a Delta infection. Other evidence finds that natural infection is better than vaccines at inducing the sort of immune response that is better at stopping upper airways infection – which is what matters for stopping transmission and getting (close) to herd immunity.
That's right, the mythical "herd immunity", or as Blakely also put it, "natural immunity".
If you let the virus wash through, natural immunity is better than vaccine immunity at protecting you against future variants. I expect that's where we'll end up going to.
Yes, Blakely is trotting out that old canard which was expected to free us of our afflictions once 60% - 70% immunity amongst the community was achieved, a number which kept ramping up higher and higher, which linguistic creativity was hoped would finally turn the trick (Blakely's "vaccine and natural infection" is actually called "super immunity" and "hyper-charged immunity" by some), which hopes were that the next wave would provide that tiny little last bit of extra immunity needed to seal the deal, if not the next wave, or the next wave, or the ne-.... you get the point.
One problem with Blakely's reference and assertion is that another study from Israel, this one published on Dec. 5th (more than three months after the study Blakely referenced was published and two weeks before The Guardian published the article from which Blakely's above quote was taken from), points out that people with this hybrid immunity-cum-"super immunity" not only can see their lauded immunity wane, but as a consequence they can once again be reinfected.
To make matters worse, the study Blakely referenced was published months before Omicron emerged (and so which at best only worked off of information pertaining to Delta), which Blakely nonetheless still chose to reference even though Omicron and its vaccine-evasiveness was out and about while he was publishing his piece.
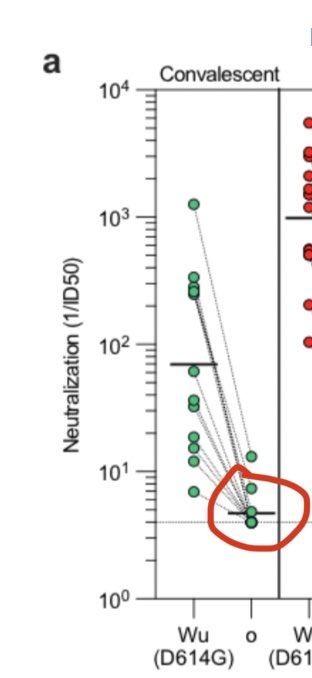
For those wondering, how might natural infection, and even the hybrid immunity of natural infection plus vaccination(s), fare in light of Omicron? Well, we don't quite know yet about hybrid immunity, but we do know that Omicron can break through natural immunity in ways that no previous COVID-19 variant ever has.
Suffice to say, and as stated by Denise Dewald, MD, and many others, "There will never be herd immunity with a virus with a genome as unstable as the coronavirus".
Otherwise, Blakely's blanket assertion of natural immunity to the Delta variant being superior to immunity provided by two doses of Pfizer to the Delta variant is much too simplistic, and thanks to several limitations in the study that Blakely references may in fact be giving Australians (and many others) the wrong idea. Not only is the sickness caused by infection less severe in those that have immunity via vaccine than in those with natural immunity via a previous infection, but according to a review (of the study that Blakely references) by Johns Hopkins Bloomberg School of Public Health,
As the authors state the primary SARS-CoV-2 variant in Israel at this time was Delta, and therefore these results may not hold for other variants. In addition, Israel only used the Pfizer mRNA vaccine, so these results may not be applicable to other vaccine platforms. One important limitation of this study, that the authors do not address, is that it is possible that some of the previously infected individuals could have had multiple SARS-CoV-2 infections before their Feb 28 cut-off. It would be more applicable to treat anyone with multiple infections as a separate group or remove them from analysis. Lastly, more granular detail on the data used would be helpful to fully assess these findings.
Secondly, a study recently published in Science showed evidence of immune imprinting by SARS-CoV-2. This derives from what immunologists call "original antigenic sin", a phenomenon whereby the immune response one's body mounts against a pathogen is akin to the response made when first encountering the pathogen, even though the pathogen being responded to is of a slightly different variant. One of the implications is that it renders Blakely's statement that "a pre-Delta variant was 13 times better than two doses of Pfizer at preventing a Delta infection" overly simplistic, due to the fact that there is no one-size-fits-all immunity conferred by the diversity of variants, some of which have greater and lesser protection against each other.
Although I'm not too keen on quoting from Murdoch rags, here's a clear explanation of the study from The Wall Street Journal.
[The] paper ... found that a person's first encounter with the virus's spike protein – the part that it uses to enter cells – be it through infection or vaccination, shaped their subsequent responses to the virus.
It detailed how, in U.K. healthcare workers, immune responses differed depending on which variant of the spike protein they first encountered. Those who were infected with the Alpha variant last winter, then vaccinated, had different immune responses to those who had been infected with the Wuhan strain during the first wave, and later vaccinated. For instance, they had stronger immune responses to the Delta strain, and weaker responses to the Beta strain, than those who had only encountered the spike protein of the original Wuhan strain. All of the authorized vaccines are based on the Wuhan strain.
“The world of SARS-CoV-2 immunity has become a very complex landscape where we’re all a little bit different, so we don’t start our vaccine with a blank sheet,” said Prof. Altmann [co-author of the study]. “This stuff needs to be decoded.”
In other words, letting oneself believe that being infected (so that one doesn't get infected?) is superior to being vaccinated is not only potentially very wrong, but also has the potentiality of very bad consequences.
To make matters worse, Blakely's suggestion to "let the virus wash through" Australians (and the rest of the world's population for that matter) is exactly what you want to do if your goal is to give the virus more opportunities to mutate and thus create yet another variant of concern, one that could very well be enormously worse than anything we've seen so far.
Moreover, what could very well be created is a variant that could not only be highly vaccine-evading and highly transmissible (like Omicron) as well as rather virulent (like both Delta and Omicron), but a variant that had all of that plus the added caveat that its vaccine-evading ability enabled it to get past the immunity characteristics that provide people with protection against severe reactions – i.e. hospitalisations and death.
But that's all fodder for another post in a few months' time, a post about what I call the Olympian variant.
Then again, perhaps that post will be invalidated, because perhaps we're all going to get lucky and this Omicron thingamajig is the last of these variant of concerns we're going to see and this whole COVID thing is simply going to... you know... peter out and become endemic like, ahem, the flu. I mean, it is possible, right?
According to Dr Julian Tang, a professor of Respiratory Sciences at Leicester University that was quoted in The Guardian,
My gut feeling is that [Omicron] is the first step in a process by which the virus adapts to the human population to produce more benign symptoms. ... I think the virus will evolve itself out of the pandemic strain very soon and become milder, more transmissible to the point where you may only need to think about vaccinating the more vulnerable members of the population.
And you know, it's not as if it was written in The Washington Post on October 31st that "The pandemic appears to be winding down in the United States in a thousand subtle ways", or that on November 8th the former FDA commissioner toldFace the Nation that "I think that we're close to the end of pandemic phase of this virus", or that it was written in The Atlantic the day after Omicron was declared a variant of concern by the WHO that "the pandemic is ending with a whimper".
December 30th, the first day every part of the USA was listed as having high levels of COVID-19 transmission (source)
In other words, when we hear CNBCsaying on December 22nd that whereas
Just weeks ago, the U.S. was on track to end the pandemic in 2022. Then, omicron hit – throwing scientists' projections into disarray.
It's actually okay because one paragraph later CNBC then states that
Now, some researchers say omicron could actually hasten the virus' transition from pandemic to endemic, albeit with large numbers of illnesses and potential deaths along the way.
The theory: Due to omicron's high rate of transmission and danger to unvaccinated and non-boosted people, hospitalizations and deaths could rise significantly in the coming weeks and months – but survivors could emerge with a degree of so-called “natural immunity” that could help protect against Covid's next variant of concern.
We can totally trust that that's a theory, and not a fantasy, right? We're gonna be protected against the next variant of concern thanks to herd immunity (or whatever the fashionable euphemism at the time is), right?
Right?
Well if you do believe that then forget bridges and step right up, cause I've got a mouthful of horse dewormer to sell you.
Sure, Tedros Adhanom Ghebreyesus, head of the World Health Organization (WHO), has stated that
2022 must be the year we end the pandemic.
And maybe it will be "ended" in 2022. Perhaps something like the Walter Reed vaccine, if actually able to successfully ward off all variants, will mean that COVID-19 will truly become a disease solely of the unvaccinated.
Then again, if Omicron does infect 3 billion people worldwide (many of whom won't be recorded to due overrun testing systems) that'd confer a rather wide population-wide immunity that could cause transmission levels to significantly drop – for a while. And for all we know such a situation could be nothing more than a case of "the calm before the storm", ushering in another "surprise" variant of concern catching the world off guard once again.
In fact, just as this piece was about to be published word was spreading about a new study led by Emma Thomson (clinical professor of infectious diseases & virologist) via the MRC-University of Glasgow Centre for Virus Research that examined the properties of Omicron versus other variants. I won't pretend to have read through it, although as it does appear that Deepti Gurdasani has we can glean from portions of her explanatory Twitter thread to elucidate things a bit.
Now to what I think is one of the most interesting insights in the paper. The preferred mechanism of entry into cells seems to have changed with omicron relative to previous variants.
There are two ways of entry into cells – delta preferentially employs fusion of the virus with the cell surface directly, while it seems omicron prefers a different mechanism to enter cells – it uses endosomes (a mechanism by which things outside the cell get taken into the cell).
What does this mean? It's hard to know. Different mechanisms of entry may have different advantages in different tissues. So it may be less able to enter cells in the lung, for example, but more able to in other tissues.
What this means for acute infection and long COVID will take time to figure out. But what's clear is that functionally and biologically omicron is very different to delta, and it's difficult to extrapolate what infection with omicron will mean – biologically.
It also highlights the huge potential for adaptation and flexibility of this virus. As the authors say: “our work demonstrates that SARS-CoV-2 exhibits high antigenic and functional plasticity; further fundamental shifts in transmission and disease should be anticipated”.
It makes it very hard to predict how this virus will evolve, and what it will adapt towards. Vitally important to adopt the precautionary principle with omicron as we understand more, and adopt suppression strategies to reduce the probability of emergence of new variants.
Which isn't necessarily bad, but nor does it sound very good. Either way, only time will tell.
In the meantime, and supposing you've even got much sovereignty and/or autonomy over your own life, it might be wise to plan accordingly. Because if a new variant does emerge later in 2022 there's a very good chance that it'll be even more transmissible than the hyper-transmissible Omicron (in order to outcompete it). But what's far from certain is what other characteristics an Omicron-on-steroids variant might bring with it. First off, will it be more virulent than Delta, and secondly, might it not only have vaccine-evading characteristics that allow it to escape vaccines, but vaccine-evading characteristics that allow it to escape their ability to ward off severe reactions (read: hospitalisations and death)? Although there's no reason to descend into outright paranoia and expect a variant of concern with the virulence of H5N1 or "simply" MERS, a hyper-transmissible vaccine-evading variant with the virulence of SARS might not be too far-fetched. If so, next year would be extremely harried, to say the least.
But regardless of what the next surprise that COVID has in store for us turns out to be, make no mistake about it – the Omicron variant is going to lay waste across the globe, and if we're lucky its case numbers will crash as fast as they grew while the carnage left in its wake – disrupted supply chains, empty supermarket shelves, shortages of all sorts, skyrocketing energy prices, stagflation, and more – won't be much worse previous waves.
That all aside, it's now time for this post's final COVID-themed and adapted Christmas carol title, John Lennon's "Happy Xmas (war is over)", which no, wasn't converted into "Happy Xmas (the pandemic is over)".
Because let's not forget: we underestimate this virus at our peril, and Omicron is nowhere near as concerning as the possible emergence of "the one we've all been waiting for".
Crappy Xmas (grandma is over)
If you did in fact have a family Christmas bash, and you did in fact decide to have grandma over, then here's to hoping that you didn't consign grandma's time to being "over".
Then again, if you did actually end up spreading Omicron to grandma and thus possibly inflicted upon her the torture of having to live out the last years of her life in misery and agony due to having developed long COVID, then yeah, grandma might just be better off if you did in fact make her "over" once and for all.
Otherwise, if you're not only actually attending a New Year's Eve party tonight but for some weird reason are inviting grandma to it, don't forget the words of Illinois governor J.B. Pritzker:
Omicron and delta are coming to your party.
Sounds of the Pandemicene, with Fanfare Ciocărlia
For those in the know it's of course all but expected that the song for this round of "Sounds of the Pandemicene, with Fanfare Ciocărlia" is no less than Urn St. Tavern (recorded with Canadian guitarist Adrian Raso, who also wrote it). Not only because a tavern is – like the super-spreading Argyle House nightclub – a place that people gather in to imbibe, but because an urn is no less than the receptacle that one's ashes are placed in after one has caught SARS-CoV-2 from a tavern-like place, died from it, and then been subsequently cremated.
Fanfare Ciocărlia & Adrian Raso – Urn St. Tavern
0:00
/246.095362
Urn St. Tavern can be found on the album "Devil's Tale", available on Bandcamp or wherever else you purchase and/or stream music from.










 Tanya Lewis
Tanya Lewis












![Reasons for Curtailing Our – and Our Childrens' – Screentime [part 2/2]](https://storage.ghost.io/c/d9/c3/d9c3ae66-3c63-49da-b4d3-18e56974e2b1/content/images/size/w680/2021/11/boy-watching-TV.jpg)










Comments